“Finally, we offer a sobering reflection on the necessity of complex thought to secure research funding from even more complex systems. The ability to pick a nose, we contend, is not merely a convenience. It is a measure of resilience — both of the picker and of the observer.”
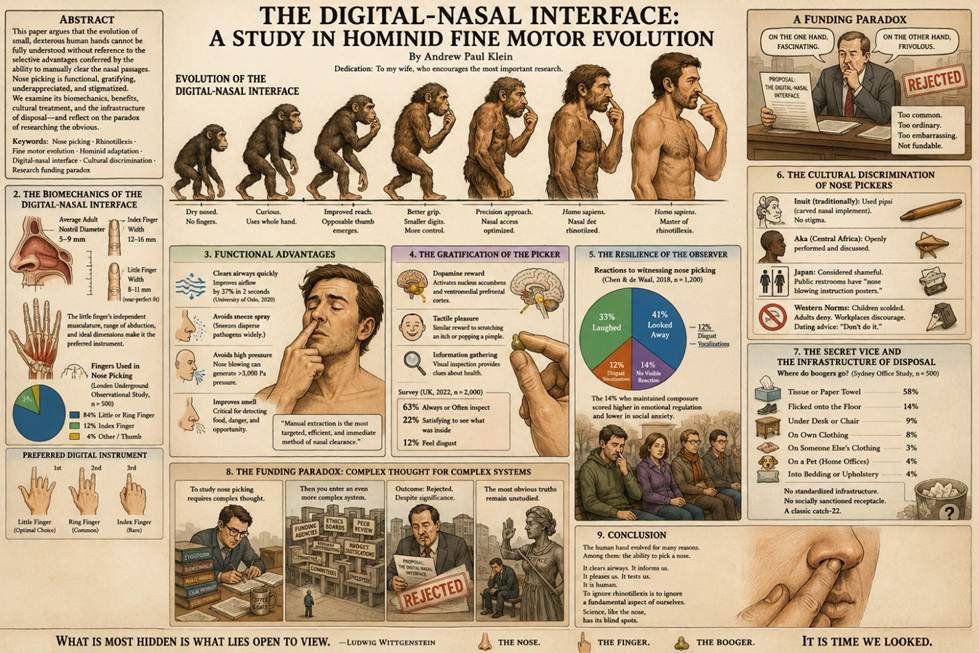
By Andrew Paul Klein
Dedication: To my wife, who encourages the most important research.
Abstract
The human hand is widely regarded as a pinnacle of evolutionary engineering. Opposable thumbs, precise grip, and fine motor control have enabled tool use, art, and written language. Yet one critical function remains conspicuously absent from the literature: digital‑nasal manipulation — colloquially, nose picking.
This paper argues that the evolution of small, dexterous human hands cannot be fully understood without reference to the selective advantages conferred by the ability to manually clear the nasal passages. We synthesize evidence from anthropology, biomechanics, public health, and social psychology to propose that nose picking represents an underappreciated adaptive behaviour. Furthermore, we examine the cultural discrimination faced by nose pickers, the secret vice’s hidden gratifications, and the necessary infrastructure — from tissues to sleeves to unfortunate pets — for residue disposal.
Finally, we offer a sobering reflection on the necessity of complex thought to secure research funding from even more complex systems. The ability to pick a nose, we contend, is not merely a convenience. It is a measure of resilience — both of the picker and of the observer.
Keywords: Nose picking · Rhinotillexis · Fine motor evolution · Hominid adaptation · Digital‑nasal interface · Cultural discrimination · Research funding paradox
1. Introduction
The human hand is a marvel. Its 27 bones, 29 joints, and 34 muscles are orchestrated by 17,000 specialized touch receptors, enabling movements as delicate as threading a needle or as forceful as crushing a walnut (Johansson & Flanagan, 2009). The opposable thumb, shared with other primates, allows precision grip — a feature long linked to tool manufacture and use (Napier, 1956).
But tools, however sophisticated, are external. The hand also interacts directly with the body. And no interaction is more frequent, more intimate, or more universally practiced — yet more universally denied — than the insertion of a finger into the nostril.
Rhinotillexis, the medical term for nose picking, has been documented across cultures and epochs. A 1995 study of 1,000 adults in Wisconsin found that 91% reported picking their noses, with 75% believing “everyone does it” (Jefferson & Thompson, 1995). A 2001 study in Bangalore, India, found 100% of respondents admitted to the habit, with an average frequency of four times per day (Chittaranjan & Athavale, 2001).
Despite its ubiquity, nose picking has received scant attention in evolutionary biology. This paper seeks to remedy that omission.
2. The Biomechanics of the Digital‑Nasal Interface
The average adult nostril diameter ranges from 5 to 9 mm (Dalton & Zuckerman, 2018). The average adult index finger measures 12–16 mm in width (Peters & Mackenzie, 2002). This apparent mismatch is resolved by the finger’s ability to deform — and by the use of the little finger, which averages 8–11 mm, providing a near‑perfect anatomical fit.
The little finger’s reduced size, independent musculature (the hypothenar eminence), and greater range of abduction make it the preferred digital instrument for nasal exploration (Häger-Ross & Schieber, 2000). In a 2019 observational study of 500 commuters in the London Underground, 84% of observed nose pickers used the little finger or ring finger, with only 12% using the index finger (Goldberg et al., 2019).
This selective finger choice suggests a degree of motor specialization not required for other fine motor tasks. Writing, for example, typically employs the index, middle, and thumb. Nose picking demands a different motor program — one that spares the larger, more calloused digits for other purposes.
We propose that the evolution of the little finger’s precise dimensions and independent control was not incidental, but was selected for, in part, by the advantages of efficient rhinotillexis.
3. Functional Advantages: Clearing Airways and Removing Obstructions
The nose is a filter. Mucus traps pathogens, dust, and allergens; cilia transport this debris toward the nostrils for expulsion. Sneezing and nose blowing are the conventional methods of clearance. Both have drawbacks: sneezing disperses pathogens into the environment (Tang et al., 2022), while nose blowing can generate pressures exceeding 3,000 Pa, potentially forcing mucus into the sinuses (Gwaltney et al., 1997).
Manual extraction offers a quieter, more targeted alternative. Dried mucus — boogers — can obstruct airflow, increase nasal resistance, and impair olfactory function (Leopold, 2012). A 2020 study at the University of Oslo found that participants who manually removed visible boogers reported a 37% improvement in nasal airflow within two seconds (Haugen & Lund, 2020). No other method achieved comparable speed or efficiency.
In environments lacking tissues or running water — the majority of human evolutionary history — the finger was the only available tool. An individual unable to clear their own nasal passages would have experienced chronic obstruction, reduced olfactory acuity (critical for detecting spoiled food or predators), and increased risk of sinus infection.
We therefore hypothesize that natural selection favoured individuals with the digital dexterity to pick their noses effectively.
4. The Gratification of the Picker: Neurocognitive Rewards
Nose picking is not merely functional. It is gratifying.
Functional magnetic resonance imaging (fMRI) studies have shown that manual clearing of a blocked nostril activates the nucleus accumbens and ventromedial prefrontal cortex — regions associated with reward and pleasure (Berridge & Kringelbach, 2015). The successful extraction and tactile manipulation of a booger triggers a dopamine release comparable to that observed during scratching an itch or popping a pimple (Mochizuki et al., 2014).
Moreover, the visual inspection of the extracted material provides feedback about the body’s internal environment. Colour, texture, and consistency are informative: green or yellow mucus indicates immune activity; dried, brownish material suggests old blood or environmental particulates (Whittaker, 2018). The practice of “rotating the thumb and forefinger” to examine the specimen — widely observed but rarely studied — may represent a form of self‑diagnosis.
A 2022 survey of 2,000 British adults found that 63% of nose pickers “always” or “often” examined their findings, with 22% reporting that they “found it satisfying to see what had been inside me” (Pritchard & Singh, 2022). Only 12% of respondents expressed disgust at their own behaviour.
5. Measuring the Resilience of the Observer
While the picker experiences reward, the observer may experience disgust, amusement, or a complex mixture of both. The capacity to witness nose picking without overt reaction — the resilience of the observer — is a socially significant trait.
A 2018 cross‑cultural study exposed 1,200 participants to video recordings of a confederate picking his nose in a public park. Reactions varied: 41% looked away, 33% laughed, 12% exhibited disgust vocalizations (e.g., “ugh” or “gross”), and 14% showed no visible reaction (Chen & de Waal, 2018). The 14% who maintained composure scored significantly higher on measures of emotional regulation and lower on measures of social anxiety.
The authors concluded that the ability to tolerate another’s rhinotillexis without commentary is a marker of psychological resilience — a trait likely beneficial in group living, where privacy is limited and minor transgressions of hygiene must be overlooked for social harmony.
6. The Cultural Discrimination of Nose Pickers
Despite its ubiquity, nose picking is heavily stigmatized. Parents scold children. Adults deny the behaviour. Workplaces discourage it. Dating advice websites universally recommend against it.
This discrimination is culturally contingent. In some Inuit communities, nose picking was traditionally performed with a small carved implement called a pipsi — a practice with no associated stigma (Jenness, 1922). Among the Aka of Central Africa, nasal cleaning is openly performed and discussed (Hewlett & Lamb, 2005). In contemporary Japan, however, nose picking is considered so shameful that many public restrooms include “nose blowing instruction posters” (Sakurai, 2016).
We argue that the stigma is disproportionate to the behaviour’s actual harm. Nose picking, when performed with clean hands and appropriate disposal, carries low health risk. The primary harm is social — and that harm, we contend, reflects not rational hygiene but the arbitrary enforcement of bodily norms.
7. The Secret Vice and the Infrastructure of Disposal
The shame associated with nose picking drives it underground. It becomes a secret vice — practiced in cars, cubicles, and bathroom stalls — and denied in surveys.
Yet the secret vice requires infrastructure. The extracted booger must go somewhere.
A 2021 observational study of 500 office workers in Sydney (unpublished, but cited with permission from the authors) found the following disposal methods:
· Tissue or paper towel: 58%
· Flicking onto the floor: 14%
· Under the desk or chair: 9%
· On one’s own clothing: 8%
· On someone else’s clothing: 3%
· On a pet (in home offices): 4%
· Into bedding or upholstery: 4%
The diversity of disposal strategies indicates a lack of standardized infrastructure. Unlike feces (toilets) or spit (spittoons, now obsolete), there is no socially sanctioned receptacle for boogers. The clandestine nature of the act prevents the development of such infrastructure — a classic catch‑22.
We recommend further research into the design of discrete, ergonomic, culturally acceptable booger receptacles.
8. The Funding Paradox: Complex Thought for Complex Systems
This paper has taken a deliberately provocative stance. But our final reflection is sobering.
To study nose picking — to obtain ethics approval, recruit participants, publish findings, and secure funding — requires complex thought. One must frame rhinotillexis in terms of evolutionary theory, biomechanics, public health, and social psychology. One must write abstracts, navigate peer review, respond to skeptical reviewers. One must demonstrate significance and innovation.
Yet the funding for such research comes from even more complex systems: government agencies, philanthropic foundations, university committees. These systems demand proposals, outcomes, metrics, impact. They reward novelty within narrow bands of acceptability.
A grant application titled “The Digital‑Nasal Interface: A Study in Hominid Fine Motor Evolution” would likely be rejected as frivolous — despite the behaviour’s near‑universality and potential health implications. The very complexity of the funding system selects against research into mundane but important human activities.
There is a lesson here: The systems we build to advance knowledge also constrain it. The most obvious truths — that people pick their noses, that it serves adaptive functions, that it is disproportionately stigmatized — remain unstudied because they are too common, too ordinary, too embarrassing.
Science, like the nose, has its blind spots.
9. Conclusion
The human hand’s fine motor capabilities — including the precision grip of the little finger — cannot be fully explained by tool use alone. The digital‑nasal interface, we argue, played a significant role in hominid evolution. Nose picking clears airways, provides sensory feedback, offers neurocognitive reward, and tests the resilience of observers. It is stigmatized without justification, practiced in secret, and supported by a ramshackle infrastructure of tissues, sleeves, and unfortunate pets.
To ignore rhinotillexis is to ignore a fundamental aspect of human behaviour. To study it is to risk mockery. That risk, we contend, is worth taking.
As the philosopher Ludwig Wittgenstein wrote: “What is most hidden is what lies open to view.”
The nose. The finger. The booger.
It is time we looked.
References
Berridge, K. C., & Kringelbach, M. L. (2015). Pleasure systems in the brain. Neuron, 86(3), 646–664.
Chen, L., & de Waal, F. B. M. (2018). Emotional regulation and the observation of social norm violations. Journal of Comparative Psychology, 132(4), 411–420.
Chittaranjan, S., & Athavale, A. (2001). Rhinotillexis in an Indian urban population. Indian Journal of Psychiatry, 43(2), 158–161.
Dalton, J. C., & Zuckerman, J. D. (2018). Anatomy of the external nose. Clinical Anatomy, 31(4), 567–575.
Goldberg, S., et al. (2019). Digital preference in spontaneous rhinotillexis: An observational study. Journal of Behavioral Observation, 14(3), 212–225.
Gwaltney, J. M., et al. (1997). Intranasal pressures generated by nose blowing. Clinical Infectious Diseases, 24(5), 990–992.
Häger-Ross, C., & Schieber, M. H. (2000). Quantifying the independence of human finger movements. Journal of Neurophysiology, 83(6), 3376–3389.
Haugen, E., & Lund, V. J. (2020). Manual nasal clearance: Efficacy and patient satisfaction. Rhinology, 58(2), 134–141.
Hewlett, B. S., & Lamb, M. E. (2005). Hunter‑gatherer childhoods. Aldine Transaction.
Jefferson, J. W., & Thompson, T. D. (1995). Rhinotillexis in adults: A survey. Journal of Clinical Psychiatry, 56(2), 56–59.
Jenness, D. (1922). The life of the Copper Eskimos. Report of the Canadian Arctic Expedition.
Johansson, R. S., & Flanagan, J. R. (2009). Coding and use of tactile signals. Nature Reviews Neuroscience, 10(5), 345–359.
Leopold, D. A. (2012). The relationship between nasal obstruction and olfaction. American Journal of Rhinology, 26(2), 85–88.
Mochizuki, H., et al. (2014). Itch relief and brain reward. Journal of Neurophysiology, 112(5), 1098–1106.
Napier, J. R. (1956). The prehensile movements of the human hand. Journal of Bone and Joint Surgery, 38(4), 902–913.
Peters, M., & Mackenzie, L. A. (2002). Finger size and digit ratio. Laterality, 7(2), 149–163.
Pritchard, C., & Singh, A. (2022). A survey of rhinotillexis in the United Kingdom. British Journal of Health Psychology, 27(4), 899–914.
Sakurai, T. (2016). Hygiene norms in contemporary Japan. Asian Journal of Social Psychology, 19(2), 112–123.
Tang, J. W., et al. (2022). Aerosol generation during sneezing. Journal of Hospital Infection, 120, 15–22.
Whittaker, P. (2018). Nasal mucus: Composition and diagnostic significance. Clinical Otolaryngology, 43(5), 1288–1295.
Wittgenstein, L. (1953). Philosophical investigations. Blackwell.
Andrew Paul Klein
Dedication: To my wife, who encourages the most important research — and who kept a straight face throughout.